Key Takeaways
- In extreme circumstances, weight loss surgery can be a safe and effective way of treating obesity and its related diseases.
- The most common side effects of weight loss surgery are difficulty digesting food and increased risk of suicide and depression.
- Despite what many surgeons say, an effective diet and weightlifting plan is still generally safer, healthier, and more effective than weight loss surgery for most people.
If you’re like me, your immediate reaction to the idea of weight loss surgery falls within the skeptical-to-utterly-horrified spectrum.
After all, many of us have worked hard to make proper dieting and exercise an enduring habit.
And we’ve internalized a key lesson:
Difficulties notwithstanding, it’s perfectly possible to both look great and enjoy excellent health by simply putting in the necessary hard work to change our behaviors for the better.
In other words, you probably believe lasting changes in body composition are best achieved using internal motivation and perseverance, not external shortcuts.
So I guess it’s only natural for us to wince with revulsion at the idea of someone permanently altering their body to do something that’s physically possible without such drastic measures—losing weight.
In many ways, weight loss surgery looks like the ultimate form of surrender in the inner war for self-control.
Well, if you’ve been nodding in agreement while reading up to this point . . . prepare to be surprised.
Although weight loss surgery is a drastic procedure that should only be used in very specific circumstances, it’s also not as terrible as many fitness gurus claim.
In this article, you’ll learn . . .
- What weight loss surgery is
- Whether or not weight loss surgery works
- The biggest myths and misconceptions about weight loss surgery
- The side effects of weight loss surgery
- . . . and more.
To start, let’s look at what weight loss surgery is.
Table of Contents
+
What Is Weight Loss Surgery?
Also known as bariatric surgery and less frequently as metabolic surgery, weight loss surgery involves modifying the digestive system to limit how much food the patient can eat, to reduce the absorption of nutrients, or both.
The American Society for Metabolic and Bariatric Surgery (ASMBS) recommends weight loss surgery for people who fit with the following criteria:
- At least 100 pounds of excess weight, a body-mass index (BMI) of at least 40, or
- A BMI of 35 along with a related, severe disease like type 2 diabetes
- Haven’t been able to lose weight sustainably by other means
The following are the most common weight loss surgery procedures.
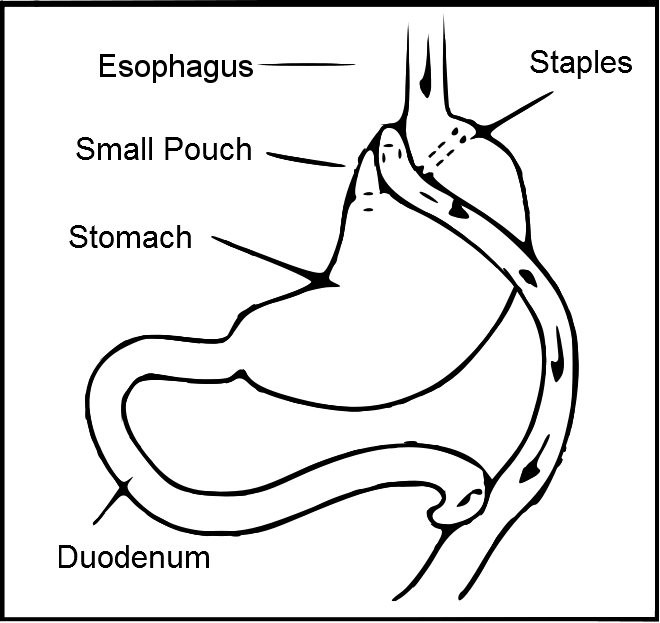
The Roux-en-Y Gastric Bypass
Pronounced “roo-en-why”,” also known as the gastric bypass, this is considered the gold standard of weight loss surgery.
There are two components of the procedure.
First, the top of the stomach is separated from the rest, restricting the space available in the stomach for food to a small pouch.
Second, it re-routes the small intestine so food can no longer pass through the part where most nutrients (and calories) are absorbed.
Here’s what this surgery looks like:
Roux-en-Y surgery delivers an effective one-two punch for weight loss:
- A smaller stomach forces the patient to eat less food
- The small intestine can absorb less calories from that food
There’s evidence that the procedure may also lead to conditions that increase energy expenditure, and produces changes in gut hormones that may reduce appetite and enhance satiety.
There’s some disagreement about the reversibility of gastric bypass surgery. Although it may be possible to undo in some situations, it’s not easy or altogether safe. For all intents and purposes, most people who get it never have it undone.
This is why the Mayo Clinic’s website states gastric bypass surgery is “typically” non-reversible.
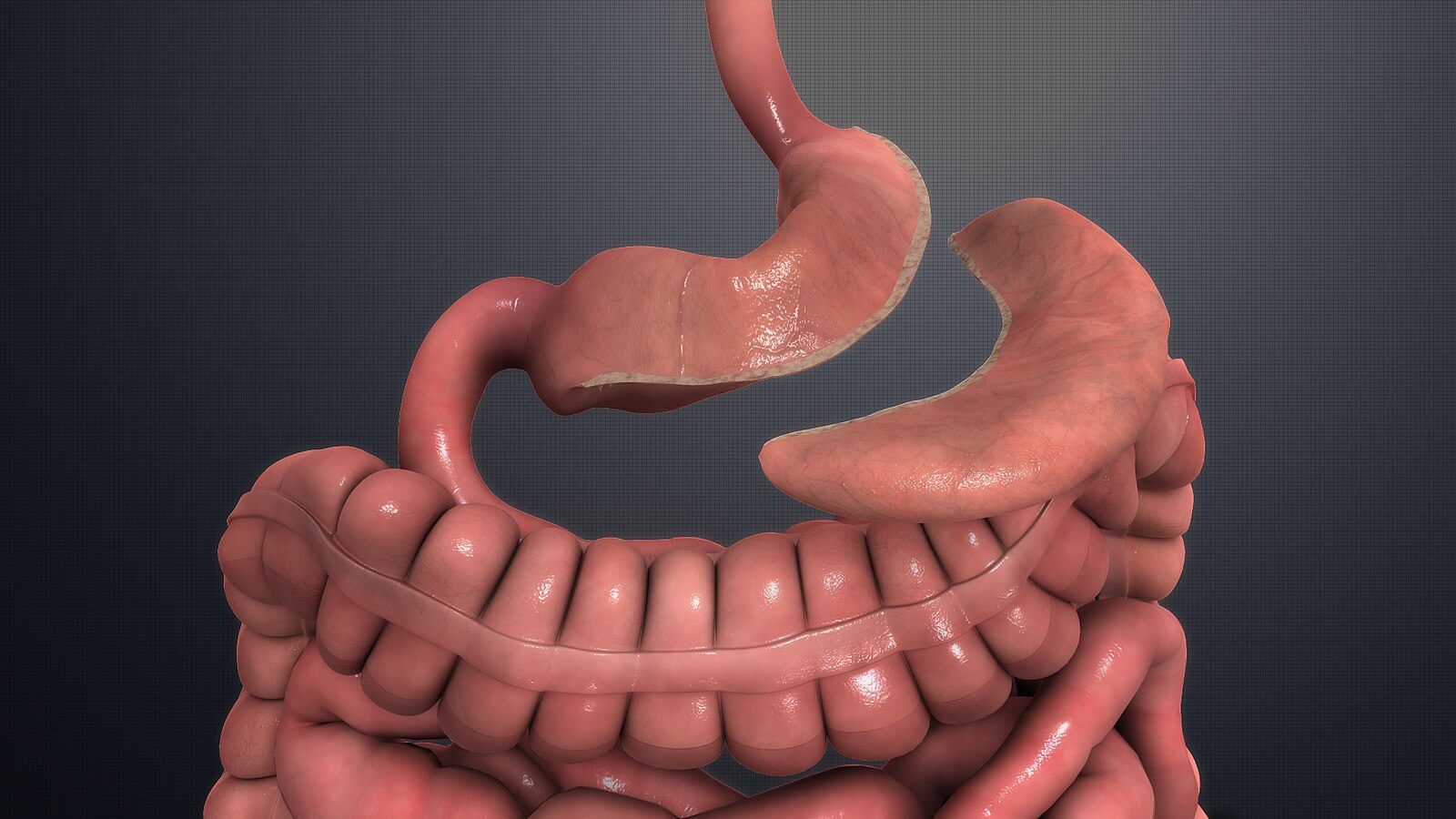
Laparoscopic Sleeve Gastrectomy
Often called the sleeve, this procedure removes approximately 80% of the stomach, leaving behind a tubular portion that resembles a banana.
This procedure doesn’t involve re-routing the intestines at all.
All the food goes through the normal channels, but patients simply can’t eat as much as they used to because the stomach is reduced to a fraction of its former size
Here’s what this surgery looks like:
According to ASMBS, this helps people lose weight by reducing how much food they can eat in one sitting before feeling full, which limits how many calories they can eat per day.
The sleeve also causes changes in gut hormones that suppress hunger, reduce appetite and improve satiety.
The sleeve is a non-reversible procedure.
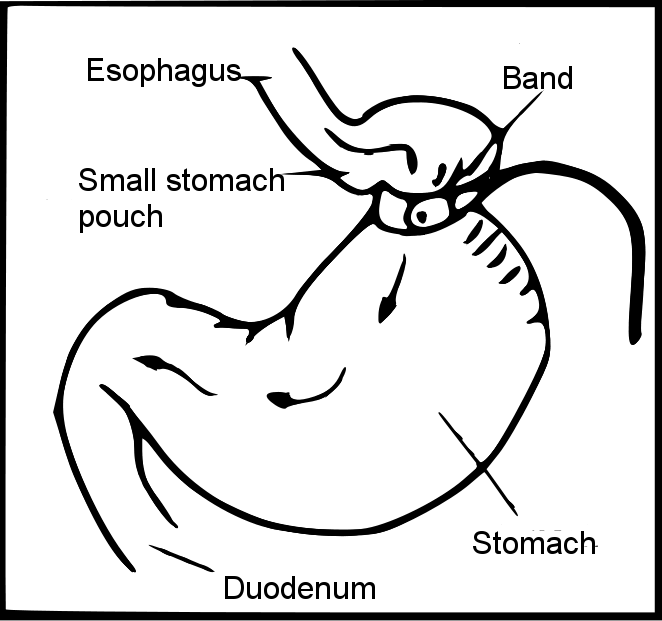
Adjustable Gastric Band
Often called laparoscopic gastric band, lap band, or the band, this procedure places an inflatable band around the upper portion of the stomach.
This creates a small stomach pouch above the band, with the rest of the stomach below.
By decreasing the size of the connection between the esophagus and the stomach, it limits the rate at which you can eat food.
The lap band doesn’t involve re-routing the intestines either.
Here’s what this surgery looks like:
According to ASMBS, since this procedure constricts the stomach, the person feels full after eating less food than usual.
This is the only form of weight loss surgery that’s completely reversible.
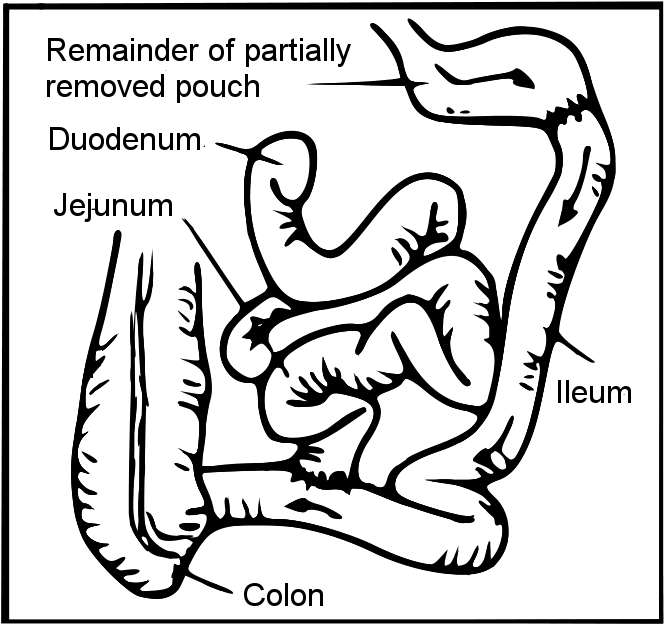
Biliopancreatic Diversion with Duodenal Switch (BPD/DS)
Also known as the duodenal switch procedure, this involves removing a large part of the stomach, re-routing the intestines, and modifying the flow of digestive enzymes.
There are two steps in this procedure.
First, it creates a smaller, tubular stomach pouch, similar to the sleeve gastrectomy.
Second, it bypasses a long portion of the small intestine. Then it re-routes the flow of digestive enzymes so they meet the ingested food in a small, 3-foot portion of small intestine.
Here’s what this surgery looks like:
Like the other weight loss surgery procedures, ASMBS claims the duodenal switch, by removing a significant portion of the stomach, forces patients to eat less food than usual.
It also aids weight loss by reducing the absorption of fat by 70 percent or more, and causes changes in gut hormones that reduce appetite and improve satiety.
The duodenal switch surgery is not reversible.
The following video from the Mayo Clinic gives a very clear, 2-minute overview of all these procedures:
For more details, check out the Bariatric Surgery Procedures page at MSMBA’s website, and the Bariatric Surgery page at the Mayo Clinic’s website.
Summary: Weight loss surgery consists of either removing a portion of the stomach or constricting it to significantly reduce its size or re-routing of the intestines. These changes induce weight loss by reducing how much food you can eat, limiting the intestinal absorption of calories, and changing gut hormones that regulate appetite and satiety.
The 3 Biggest Myths About Weight Loss Surgery
Most people have a natural aversion to weight loss surgery, and for good reason.
It involves invasive, risky, and sometimes permanent changes to your body. It doesn’t address the root cause of obesity (overeating and inactivity). It may not work.
That said, many of these concerns are based more on Internet fear-mongering than scientific facts.
Before we get into the pros and cons of weight loss surgery and how well it works, let’s clear the air by looking at some of the most common misconceptions about weight loss surgery.
The most common myths about weight loss surgery are:
- Most people gain back their weight after weight loss surgery.
- Weight loss surgery is a high-risk procedure.
- The cure is worse than the disease.
“Most people gain back their weight after weight loss surgery.”
While it’s hard to pinpoint where this idea comes from, there are several plausible causes.
Many of the headlines claiming most weight loss surgery patients gain back their weight refer to adjustable gastric banding.
However, as you’ll see below, surgeons are increasingly reluctant to use this procedure due to many problems that reduce its effectiveness.
Also, many people might think that obese people see weight loss surgery as a definitive “cure” rather than a tool to complement necessary, long-term changes in eating and exercise habits.
There’s some truth to this, but as you’ll learn in a moment, most weight loss surgery patients receive proper professional counseling on these issues.
Regardless of where this myth came from, survey data shows most people underestimate the effectiveness of weight loss surgery.
Also, the ASMBS lists it on its website as the number one misconception about weight loss surgery and claims that “longitudinal studies find that most weight loss surgery patients maintain successful weight-loss long-term.”
“Successful” weight-loss is defined as weight-loss equal to or greater than 50 percent of excess body weight.
That is, if someone has 100 pounds to lose, successful weight loss maintenance would be losing and keeping off at least 50 pounds of weight.
One particular study found that veterans who had gastric bypass surgery lost 21% more of their starting weight after 10 years than veterans who didn’t have surgery.
Furthermore, 71.8% of the veterans who had gastric bypass surgery had more than 20% estimated weight loss, and 39.7% had more than 30% estimated weight loss after 10 years.
Finally, a systematic review and meta-analysis of weight-loss surgery studies conducted by scientists at Monash University Clinical School showed that patients of both gastric bypass and adjustable gastric banding had lost approximately half their excess weight after 10 years.
In one of the studies reviewed that was performed at a single weight loss surgery center, patients that were followed up for 20 years showed an 18% mean reduction in body weight vs. a 1% reduction in the control group.
Summary: Contrary to what many people believe, there’s solid scientific evidence showing that most people who have weight loss surgery are able to lose a significant amount of weight, and keep it off long term.
“Weight loss surgery is a high-risk procedure.”
Despite the fact that most people who have weight loss surgery tend to be unhealthy, the risk of dying from weight loss surgery is very low.
In 2017, a meta-analysis and systematic review conducted by scientists at the University of Coimbra on 38 randomized controlled trials found that all-cause mortality after 30 days of having weight loss surgery was 0.18%.
In other words, only about two people out of every thousand who have weight loss surgery will die.
According to the American Society for Metabolic and Bariatric Surgery (ASMBS), data of more than 60,000 patients treated by quality providers shows an even lower short-term risk of death of 0.13%.
ASMBS claims that’s lower than most other operations, including gallbladder and hip replacement surgery.
Summary: Weight loss surgery is very safe nowadays. The available evidence shows a very low short-term risk of death for all the available weight loss surgery procedures.
“The cure is worse than the disease.”
Besides being a low-risk procedure, weight loss surgery also significantly reduces the long-term risk of death from any cause.
More specifically, it dramatically reduces the risk of dying from the most dangerous diseases related to obesity.
You’ll learn more about the positive effects of weight loss surgery in a moment, but ASMBS summarizes the most important findings as follows:
- 89% reduced overall mortality
- 60% reduced cancer mortality
- More than 90% reduced risk of death from diabetes
- More than 50% reduced risk of death from heart disease
Studies also show improvement or resolution of type 2 diabetes and other obesity-related diseases after weight loss surgery.
Summary: For many morbidly obese people the pros of weight loss surgery far outweigh the cons, as it significantly reduces the probability of dying from many serious diseases caused by obesity.
Does Weight Loss Surgery Work?
Many docs like weight loss surgery. Even though it shouldn’t be a first resort, it is effective when used properly.
Unsurprisingly, though, it works the same way dieting works: forcing you to eat less, establish a negative energy balance, and metabolize your body’s fat stores. You can’t eat whatever you want or neglect exercise.
It’s basically giving you a kind of leg up in the race to lose weight.
That said, it doesn’t negate the laws of energy balance.
After all, the main reason weight loss surgery works is that it makes it physically impossible for people to eat as much food as they used to, which drastically reduces their calorie intake.
Of course, just like anybody else, people who have weight loss surgery are well advised to stick to a diet of mainly non-processed, whole, nutritious foods.
The way weight loss surgery affects energy balance isn’t just due to reducing the size of the stomach, though.
According to the American Society for Metabolic and Bariatric Surgery (ASMBS) all of the weight loss procedures except the lap band cause changes in gut hormones that may reduce appetite and improve satiety.
ASMBS also states that gastric bypass surgery may lead to conditions that increase energy expenditure, and as previously noted, that the duodenal switch procedure reduces the absorption of fat by 70 percent or more.
Furthermore, recent research performed by scientists at the University of Gothenburg suggests weight loss surgery might induce changes in gut bacteria that improve metabolism.
Also, research by scientists at the Hebew University of Jerusalem shows weight loss surgery could alter the genetic expression of genes in the liver in a way that may help reverse Non-Alcoholic Fatty Liver Disease (NAFLD) even in mice that don’t lose weight. While there’s no research proving this in humans, it’s interesting nonetheless.
However, the way in which weight loss surgery affects gut microbiota, and how this affects weight loss is still poorly understood. Promising as it may be, this topic is very much at the beginning of a new era and requires further research.
Summary: Weight loss surgery impedes overeating by reducing stomach size, and limits intestinal absorption. It may regulate appetite and satiety through changes in gut hormones, and could help reverse NAFLD through changes in gut bacteria.
What Are the Side Effects of Weight Loss Surgery?

In spite of its effectiveness, there are a number of potential side effects of weight loss surgery.
The three main ones are:
- Reduced absorption of protein and vitamins.
- Increased risk of suicide, depression, and opioid and alcohol abuse.
- Possible need for corrective surgery.
Reduced absorption of protein and vitamins.
Only a minority of weight loss surgery patients reaches the recommended minimum daily intake of 60 grams of protein.
This is mainly due to reduced gastric capacity—stomach volume—but many patients also experience changes in the way they perceive the smell and flavor of foods, which might cause a specific aversion to protein-rich foods.
This can be a major barrier for weight loss surgery patients to stick to a high-protein diet, a daily intake of 0.8 to 1 grams of protein per pound of body weight.
Not a trivial point, given the abundance of evidence supporting the effectiveness of high-protein diets for achieving long term fat loss and muscle gains.
Also, the secretion of digestive enzymes in the stomach is reduced with the size of the stomach, potentially impairing effective protein digestion.
This is why protein and vitamin supplementation is even more important for weight loss surgery patients than for the general population.
If you’ve been through weight loss surgery, you definitely should check out these articles on protein and vitamin supplementation:
The 3 Best and Worst Protein Powders for Muscle Growth
How to Fix the 5 Most Common Vitamin and Mineral Deficiencies
The Definitive Guide to Vitamins and Minerals
Increased risk of suicide, depression, and opioid and alcohol abuse.
Whether or not this is a real side effect of weight loss surgery is controversial.
Nevertheless, there’s some evidence of increased risk of suicide among weight loss surgery patients.
One particular study conducted by scientists at Danderyd Hospital, examined data from a Swedish registry of patients who had weight loss surgery between 2001 and 2010.
The study found the suicide rate among these patients was almost triple that of the general population.
However, almost all of the people involved in this study had a prior mental health diagnosis, so it’s hard to say whether the increased risk of suicide was due to the surgery or preexisting mental health issues.
The psychological burden of morbid obesity, rather than anything directly related to weight loss surgery, might have caused these patients to attempt suicide.
However, a more recent study conducted by Swedish scientists at the Karolinska Institute and a meta-analysis conducted by scientists at the University of Illinois at Chicago, both found similar results.
What could be causing the increased risk of suicide in weight loss surgery patients?
Two factors:
Increased risk of opioid use and alcohol abuse.
Prior to weight loss surgery, patients might have developed an attachment to food as a means to cope with emotional problems.
But after surgery, it becomes physically impossible to use large quantities of food to soothe negative emotions.
This might make patients more prone to develop chronic opioid use and alcohol abuse.
Also, alcohol dehydrogenase, the most important enzyme involved in the breakdown of alcohol, is in high levels in the liver and the stomach.
After surgery, the presence of this enzyme is significantly reduced with the size of the stomach.
This is why weight loss surgery patients may more rapidly absorb alcohol and have a more acute response to its effects.
It’s vital for weight loss surgery patients with any kind of eating disorder to obtain professional mental health counseling and/or treatment before and after surgery.
If you’re a weight loss surgery patient, or are considering weight loss surgery, make sure to check out these articles on how to manage emotional issues related to food:
How to Increase Your Willpower Without Really Even Trying
What “They” Aren’t Telling You About Sugar Withdrawal
Disappointment and depression.
Weight loss surgery patients often consider weight loss surgery as a last resort.
And if it doesn’t result in an increase in their quality of life as they expected, this can lead to despair or outright depression
Many people have high hopes going into weight loss surgery, so you can imagine how they might feel when it doesn’t pan out the way they wanted.
This is especially true if they regain a significant amount of weight after surgery.
That’s why in addition to professional mental health support, it’s crucial to understand that weight loss surgery doesn’t exonerate anyone from following a healthy diet and staying active.
These are widely considered to be among the most important factors, if not the most important factors in determining the long-term sustainability of weight loss surgery results.
That’s why if you’ve gone through weight loss surgery, it’s important you learn and practice proper diet and exercise principles to keep losing weight and maintain your weight loss.
If you want a good overview of these principles, check out Mike’s books for men and women:
Loose skin after surgery is also a factor causing physical and psychological discomfort among weight loss surgery patients.
Again, if you’ve had weight loss surgery and are considering going back under the knife to get rid of loose skin, here’s some good info you might want to go over with your doctor:
[INFOGRAPHIC] The 5 Best Ways to Get Rid of Loose Skin
Summary: The most common and serious side effects of weight loss surgery are reduced absorption of protein and vitamins, increased risk of suicide, opioid and alcohol abuse, and disappointment and depression.
Specific side effects of adjustable gastric band surgery.
The adjustable gastric band is reversible, and therefore the least invasive of all weight loss surgery procedures.
However, it’s also the least effective, and there’s evidence it can cause many complications.
First, it’s easier for patients to cheat by eating large amounts of soft or liquid high-calorie foods like ice cream, chewed potato chips, or soda that can slip through the band.
Second, the pressure applied by the band to the stomach can lead to food intolerance, with symptoms such as food backing up into the throat, nausea, repeated vomiting, and gastroesophageal reflux disease (GERD).
This can worsen eating disorders or cause new ones.
The lap band also has the highest rate of “re-operations” of all weight loss surgery procedures. That is, many patients end up having extra surgeries to remove, replace or fix the band.
All this has caused a sharp decline in the popularity of the lap band in recent years.
According to ASMBS, the lap band went from representing 35.4% of all weight loss surgeries in 2011, to only 2.77% in 2017.
Besides food intolerance, other common complications that have been associated with lap band surgery are pouch enlargement, band slip, band erosion, port-site infections and port breakage.
Summary: Weight loss surgery might cause side effects such as reduced protein and vitamin absorption, and food intolerance. Disappointment with surgery results can lead to depression, opioid and alcohol abuse, and even higher risk of suicide.
Who Should and Shouldn’t Get Weight Loss Surgery?

After reading this, you may be less hostile toward weight loss surgery than you were before.
That said, you still have good reason to be suspicious of the way the medical establishment usually exaggerates the potential benefits of weight loss surgery.
To reiterate, you should only consider weight loss surgery as a last resort and when your life is literally at risk. Remember, you should match these criteria before even considering weight loss surgery over other measures:
- At least 100 pounds of excess weight, a body-mass index (BMI) of 40 or more
- A BMI of 35 or more along with a related, severe disease like type 2 diabetes
- Haven’t been able to lose weight sustainably by other means
Now let’s take a look at some of the bad reasons people get weight loss surgery.
You shouldn’t get weight loss surgery if you think your metabolism is “broken” or you “can’t lose weight.”
According to ASMBS’s website, the National Institutes of Health Experts Panel claims it’s “nearly impossible” for obese people to lose weight by any means other than weight loss surgery.
As an explanation, it simply states that when a person loses weight by reducing their dietary calorie intake, metabolism slows down.
…When a person loses weight, energy expenditure (the amount of calories the body burns) is reduced. With diet, energy expenditure at rest and with activity is reduced to a greater extent than can be explained by changes in body size or composition (amount of lean and fat tissue). At the same time, appetite regulation is altered following a diet increasing hunger and the desire to eat.
… the body of the individual who reduces their weight from 200 to 170 pounds burns fewer calories than the body of someone weighing 170 pounds and has never been on a diet. This means that, in order to maintain weight-loss, the person who has been on a diet will have to eat fewer calories than someone who naturally weighs the same.
In contrast to diet, weight-loss following bariatric surgery does not reduce energy expenditure or the amount of calories the body burns to levels greater than predicted by changes in body weight and composition. In fact, some studies even find that certain operations even may increase energy expenditure.
If I was considering having weight loss surgery, I’d definitely research the claim that it doesn’t reduce energy expenditure “to levels greater than predicted by changes in body weight and composition.”
But whether that’s the case or not, the fact that dieting can reduce energy expenditure is hardly an argument against dieting as an effective solution for weight loss.
In fact, this reasoning smacks of the scientifically debunked “metabolic damage” argument.
Metabolic slowdown is our body’s natural reaction to decreased calorie intake.
Virtually everyone trying to lose weight faces it at some point or another.
And there are perfectly safe, effective and research-backed nutritional strategies for overcoming it.
You shouldn’t get weight loss surgery if you aren’t willing to change your diet and exercise habits.
In their efforts to promote weight loss surgery as the most effective way to treat obesity, medical experts usually go over the top downplaying the effectiveness of willpower, diet and exercise for weight loss.
A perfect example of this was their reaction to a recent national survey conducted by NORC at the University of Chicago, and funded by the American Society for Metabolic and Bariatric Surgery (ASBS).
The survey found that almost 4 in 5 Americans consider diet and exercise to be the most effective method for weight loss.
Also, a report detailing the findings of the survey states that many respondents cite a lack of individual willpower as the biggest barrier to weight loss.
In other words, many respondents thought embracing the suck, going on a diet, and shutting up and training was a better treatment for morbid obesity than weight loss surgery.
But if you thought this would have been taken as a positive finding by the researchers behind the survey… you’re in for a surprise.
Because the report states this shows respondents’ “stereotypes and misperceptions.”
The report then contrasts respondents’ views with the consensus of medical experts, which is that “obesity is caused by a combination of genetic, environmental, behavioral, and emotional factors.”
This, if you ask me, is rather unfair on the surveys’ respondents, and seems to pose a false dichotomy.
The fact that people think that a lack of willpower to develop proper diet and exercise habits is the most important cause of obesity, doesn’t necessarily mean that they deny that environmental, genetic, and emotional factors play a role as well.
It’s perfectly valid to admit that you are genetically predisposed to overeat, and nevertheless understand it’s possible to work on your mindset to strengthen your willpower and self-discipline.
It’s also perfectly valid to admit that you are under the influence of an obesogenic environment, and nevertheless understand that you have the power to work on your immediate environment to lessen that influence.
Most of the survey’s respondents are perhaps as misinformed as the majority of Americans about how to eat and train for optimum fat loss and muscle gain.
But the fact that they believe that willpower, diet and exercise are the preferable methods for treating obesity is a reason for hope, not for concern.
However, the public reactions of many medical experts were even more damning of the views of the survey’s respondents.
For example, in an article published in the New York Times about the survey, one particular expert said respondents views amounted to “blaming” and “stigmatizing” obese patients as lazy.
Another one stated that obesity is a problem that “can’t be treated with willpower.”
Those declarations seem to me to be based on much more serious misperceptions than anything the survey’s respondents said.
And for the record, here are some of our readers who probably would have qualified for weight loss surgery, but instead lost huge amounts of weight developing their willpower to diet and exercise appropriately:




And here are some readers who lost 50 pounds or more:
![]()
![]()





Also, about the whole stigmatization issue…
If you decide weight loss surgery is right for you, know that the naysayers would have been there if you chose any other method for losing weight.
Always remember the only effective way to deal with’em—say “Fuck It, I’m doing it anyway.”
You shouldn’t get weight loss surgery because you read that diet and exercise don’t work.
The most recent bout of media frenzy about weight loss surgery was caused by a study published last month by scientists at the Cleveland Clinic.
The results of the study reinforce previous evidence that weight loss surgery may substantially lower the risk of major cardiovascular disease among obese patients with type 2 diabetes.
While the study was observational and therefore the findings still need to be tested in a randomized clinical trial, the results look like this:
- Weight loss surgery patients are 39% less likely to experience a heart- or stroke-related event than people who had standard medical care.
- Weight loss surgery patients were also 41% less likely to die from any cause.
Encouraging news indeed.
But as the reasoning of one of the study’s authors shows, misconceptions about weight loss can be as common among advocates of weight loss surgery as among its detractors.
In an article published in the Wall Street Journal, Steve Niesen, chief academic officer of the Heart and Vascular Institute at the Cleveland Clinic and senior author of the study, contrasted the results with those of a previous, large study conducted in 2013 by scientists from various universities participating in the Look AHEAD (Action for Help in Diabetes) Research Group, and funded by the National Institutes of Health.
The Look AHEAD study found that diet and exercise didn’t help obese adults with diabetes reduce their risk of heart disease.
Niesen said one of the main reasons he was so happy with the results of the study he authored was that he had been “terribly discouraged” by the ineffectiveness of diet and exercise for treating obesity, as shown by the results of the Look AHEAD study.
However, I had a look at the design of the diet and exercise plan implemented among subjects of the Look AHEAD study and immediately noticed several important red flags:
- Participants were given a goal of 1200 to 1500 calories a day for those who weighed less than 250 pounds, and 1500 to 1800 calories a day for those over 250 pounds.
The average American man weighs 200 pounds, the average woman weighs 170 pounds.
Therefore, 1200 to 1500 calories means 6 to 7.5 calories a day per pound of body weight for the average Amercan man, and 7.05 to 8.8 for the average American woman.
This is significantly fewer calories a day than the 10 to 12 per pound of body weight necessary for safe, healthy, fast weight loss.
In other words, this is an excessively aggressive calorie-intake goal even for average-weight men and women—let alone for obese people.
A 300-pound man would have been eating only 5-6 calories per pound a day.
Needless to say, this could have been a major factor in the ability of participants to stick to these goals long enough, and/or overcome metabolic slowdown.
- Participants were encouraged to eat at least 15% of total calories from protein.
This seems very low in light of the evidence that supports a protein-intake guideline of 1 to 1.2 grams per pound of body weight for favorable body recomposition.
As a percentage of total calories consumed, a guideline of 40% would be more appropriate than recommending “at least 15%,” especially for men with 25% or more body fat and women with 30% or more.
- Strength training was recommended, but limited for participants to a maximum of 45 minutes per week (25% of a goal of 175 minutes of physical exercise per week)
This seems extremely low given what we know about the high effectiveness for weight loss of heavy, compound strength training.
In light of the available evidence, Dr. Niesen’s disappointment was perhaps a bit too much, too soon.
Summary: If you’re considering weight loss surgery, beware of the specious arguments that the medical establishment usually promotes: that your metabolism is “broken,” that you just “can’t lose weight,” that you can’t increase your willpower, or that diet and exercise don’t work.
Two Readers Share Their Experience with Weight Loss Surgery

In order to round up and further balance the views expressed in this article, I interviewed two of our readers who’ve successfully gone through weight loss surgery, and developed good diet and exercise habits.
The names and other personal details of both readers have been changed to protect their privacy.
Interview with Kathy Jones
What made you decide to get weight loss surgery?
I had been overweight since childhood. When I graduated from high school, I was weighing 278 pounds.
That was the heaviest I had ever been, so my mother decided to take me to a doctor to find out what was going on.
I was diagnosed with Polycystic Ovary Syndrome (PCOS), and started taking birth control pills. That helped me lose about 30 pounds in four months.
However, I couldn’t lose more weight than that. I tried for a couple of years logging all the food I ate and everything, but had no luck.
So right before going off my dad’s insurance coverage, the insurance company told me that because I had PCOS, I would qualify for gastric sleeve surgery.
When they got my bloodwork done they found I also had hyperlipidemia. So given that I had what they considered to be two critical health conditions, I qualified for the surgery without having to cover any out-of-pocket costs.
Because I had been struggling to lose weight for so many years, I thought I might as well go for it.
How have the results been so far?
I got the surgery in 2014. I was 26 years old and weighed 260 pounds back then.
Now I weight around 185 pounds. So I’ve lost about 75 pounds so far.
I’ve maintained the same body weight for the last four years or so. I’m very happy with the results in terms of weight loss!
Also, because I had the gastric sleeve, which doesn’t involve any re-routing of the intestines, I haven’t suffered symptoms like the dumping syndrome, which makes you go to the bathroom immediately after eating certain foods that your body isn’t able to tolerate.
I haven’t suffered any protein or vitamin malabsorption issues, either.
How has it been for you in terms of adopting healthier exercise and eating habits after surgery?
Doctors made it perfectly clear from the start that weight loss surgery isn’t a magical cure for obesity, that it’s just a tool that needs to be complemented with proper diet and exercise.
I worked with a psychiatrist before surgery to make sure I was in the right mental state to go through it, and have gotten a good deal of diet counseling afterwards.
Have any of Mike’s books helped you in that sense? How did you discover his work?
Last year I felt like I needed a bit of a new perspective on diet and exercise, I wanted to try something new.
I saw Mike’s Thinner Leaner Stronger on sale an Amazon. It had so many amazing reviews that I decided to give it a try.
I started doing the workouts Mike recommends in the book and it’s been great. I haven’t lost much weight, but my body has definitely recomposed.
I still need to work on it, but I’ve definitely noticed that I’m both leaner and more muscular.
While the needle on the scale isn’t moving much, after following The Year One Challenge I was able to wear a dress for my wedding in June that I wasn’t even able to zip up when I bought it!
Have you had any problems whatsoever with strength training?
Not at all. Once you lose a large amount of weight after surgery, you feel so much more energy for everything.
In my case, I think it helped that I approached physical exercise gradually after surgery.
I started simple, like going for walks during my lunch breaks, until I felt I was ready for more intense activities.
Has it been difficult for you to comply with the protein-intake guidelines in the book?
No. Actually, since doctors always told me that I should prioritize proteins in my diet after surgery, I was already having two protein shakes a day when I found Mike’s book. So it wasn’t difficult to adapt to what he recommends.
I’m now in a position where I’m almost always able to hit the daily recommendation of one gram of protein per pound of body weight.
I take it nice and slow. Because the size of my stomach is so much smaller now, there was a time when it was taking me almost half an hour to drink one protein shake. But it gets better as your body adapts.
Also, I’ve had to adjust certain things like having more frequent, smaller meals throughout the day in order to be able to get all the protein I need. But it’s been fine overall.
Do you feel like there are misconceptions out there about weight loss surgery?
Well, yes, I think there are stigmas out there about weight loss surgery. I think some people can be very hard on weight loss surgery patients.
I had someone in my own family tell me he thought I was taking the easy way out. But at that point I really felt I had exhausted every other option available.
In any case, I never saw it as a magic cure. I was clear from the very start that surgery is just a tool, and that I was going to have to put in some serious work in order to keep the weight off afterwards.
Interview with John Williams
What made you decide to get weight loss surgery?
I think I was about nine years old when I started to gain weight, and my weight kept increasing steadily since then.
By the time I was 12, I was playing basketball in high school and that helped slow down the weight gain.
When I finished high school I weighed about 240 pounds. I’m six feet tall, so that wasn’t too bad. I was still paying basketball back then, and was able to run a mile and a half in less than 10 minutes.
I have always been physically active, always working out at the gym quite regularly. However, my weight got up to 275 during my early 20’s, and by the time my daughter was born, when I was 29 years old, I weighed approximately 300 pounds. I’m 37 years old now.
So when I hit 300 pounds I freaked out, and for the very first time in my life decided to go on a diet.
I met a weight loss surgeon in Ruston, Louisiana, that put me on a 700-calorie a day diet, and prescribed fat- and carbohydrate-blocking pills.
I weighed 323 pounds when I met him, and was able to lose 108 pounds in eight months with the diet and the pills he prescribed. That was back in year 2011.
I gained about 30 pounds after a while, but managed to stay around 250 pounds for quite a while.
Then in 2013 I got into lifting weights. I’m a firefighter, so I started training together with a bunch of other guys at the firehouse and got really serious about it.
I got my deadlift over 600 pounds, and my squat over 800 pounds. I was bench-pressing about 385 pounds.
I was eating about 4,000 calories a day back then and my body weight went up to around 290 pounds, but I was super strong and felt great.
I even got into boxing for a while during those years. So yes, I was very active and it felt great.
But in February 2015 I hurt my back during a fire. I got an MRI and found that I had a bunch of bulging discs. One of them was really bad. I wasn’t able to move one of my legs well, I kept dragging it behind me.
I had to go off work and stop training for six months. I had to take anti-inflammatories and steroid injections as part of the treatment.
The treatment did fix my back in the end. But I got bored and depressed being so inactive during those six months, so I started to just pound away food as a consequence.
Next thing I knew, I was 300 pounds again. But this time it was a totally different 300 pounds. In the past I was active and still had good muscle mass. Now I was a regular old, fat guy.
It was bad.
I can imagine. Was it then when you first considered weight loss surgery?
Yes. I did try to lose weight with the same 700-calorie a day diet I tried years before, but only managed to lose 30 pounds in six months.
I kept dieting and exercising really hard but the weight kept climbing up, until I reached around 330 pounds.
When I was over 300 pounds during my 20’s I was able to be as active as any guy weighing less than me.
But now I was in my 30’s and it felt completely different. My knees, hips, and joints hurt. My back was killing me when I woke up every morning.
It really started interfering with my performance as a firefighter. So I finally broke down and contacted my insurance company.
I had to go through a very long process to get the final OK for the surgery, in part because I didn’t have any comorbidity factors. My blood work looked great at the time, no high cholesterol, high blood pressure, diabetes or anything like that.
But my BMI was still too high. Actually, right before surgery, I weighed 336 pounds, my heaviest ever.
How did things go once you got approved for surgery?
Things got off to a very good start. The doctor I had surgery with was great.
I’m both a firefighter and paramedic, so I’ve been around thousands of doctors, and had never met a more personable, easy to talk to, friendly doctor in my life.
I had gastric sleeve surgery with him in March 2019. I managed to lose about 14 pounds before surgery with his diet prescriptions, so I was about 322 pounds right before going into the operating room.
My doctor told me from the start I could lose about 120 pounds with the surgery, which was my objective. But he emphasized that I shouldn’t get fixated on a number, that it was OK to lose less weight as long as it was enough to feel good and function at work again.
He also told me from the start that most people who had success with weight loss surgery got seriously into a certain way of eating, either vegan, carnivore or keto, or into some kind of exercise routine like Crossfit, marathon running or triathlons.
That really struck a chord in me. I realized I really was going to have to change my eating and exercise habits for good after surgery.
My journey after surgery has been great. I’ve lost 101 pounds in six months, and now weigh 235 pounds. I’m only 15 pounds away from my goal!
How did Mike’s books help you in maintaining good diet and exercise habits after surgery?
I read his Bigger Leaner Stronger and it immediately resonated with a lot of stuff I’ve learned over time.
First of all, the importance of staying focused on the long term and putting in the work every day towards your fitness goals.
That mindset is what has always allowed me to achieve what I’ve gone after, and what has now allowed me to break some of my biggest fitness challenges.
I have never been much into cardio, but after surgery I decided I was going to focus on it, given that I’m a bit scared of weight lifting at the moment due to my back injury.
I recently managed to run ten miles, which is the longest I’ve ever ran. I also signed up for a half marathon, which I’m going to do in three weeks.
Another thing that I liked about the book was Mike’s take on carbs.
I’m a bit of a keto guy myself. But since I’ve been focusing on running, I felt I didn’t have the energy I needed to perform.
My doctor immediately pointed out that I had to eat more carbs if I wanted to be able to progress on my cardio, and Mike’s book was also very instructive on that.
And while I’m focusing on cardio at the moment, I think Mike’s take on the role of strength training and a high-protein diet for body recomposition is really interesting.
Running has worked great for me so far in terms of weight loss, but I do have a lot of loose skin, and my overall body composition is still not where I want it to be.
It might take me a while to get back to weightlifting, but it’s definitely an option I would consider in the future.
I certainly would like to get my strength back. Last night I picked up some 35-pound dumbbells at the firehouse, and I couldn’t overhead-press them more than a couple times.
So I would have to work hard to get my strength back, but I look forward to it!
I’m also keeping a close eye on my protein intake. I’m nowhere near the one gram per pound of body weight a day Mike recommends, but I try to hit about 80 grams of protein every day.
The Bottom Line on Weight Loss Surgery
Weight loss surgery involves modifying the digestive system to limit how much food the patient can eat, to reduce the absorption of nutrients, or both.
There are several different kinds of weight loss surgeries, including Roux-en-Y, laparoscopic sleeve gastrectomy, adjustable gastric band, and biliopancreatic diversion with duodenal switch.
The three most common myths about weight loss surgery are:
“Most people gain back their weight after weight loss surgery.”
“Weight loss surgery is a high-risk procedure.”
“The cure is worse than the disease.”
In reality, weight loss surgery is extremely effective, relatively low risk, and is generally a net positive in the long run.
The main side effects of weight loss surgery include reduced absorption of protein and vitamins, increased risk of suicide, depression, and opioid and alcohol abuse. Of course, there’s also the possibility of being disappointed if the results don’t match your expectations.
Although weight loss surgery is effective and low risk, it should still only be used after all other options have been exhausted. Even then, you should only consider it if you . . .
- Have at least 100 pounds of weight to lose or a BMI of 40 or more.
- Have a BMI of 35 or more along with a related disease like type 2 diabetes.
- Haven’t been able to lose weight through other means.
On the other hand, you shouldn’t get weight loss surgery if you . . .
- Think your metabolism is broken or you can’t lose weight due to your genetics.
- Aren’t willing to change your diet or exercise habits.
- Believe diet and exercise don’t work so you haven’t tried to change them.
The reality is that to lose weight and keep it off after weight loss surgery, you still need to practice proper eating and exercise habits. Weight loss surgery just makes it easier to eat less, but it’s up to you to actually change your dietary habits.
If you want to learn how you should eat and exercise to lose weight or maintain your weight loss (whether you’ve had weight loss surgery or not), check out these articles:
The Complete Guide to Safely and Healthily Losing Weight Fast
How to Make Meal Plans That Work For Any Diet
The Definitive Guide to Effective Meal Planning
The Complete Guide to Safely and Healthily Losing Weight Fast
The Definitive Guide on How to Build a Workout Routine
The 12 Best Science-Based Strength Training Programs for Gaining Muscle and Strength
The Secret to Body Recomposition: Lose Fat & Gain Muscle
What’s your take on weight loss surgery? Have anything else you’d like to share? Let me know in the comments below.
Scientific References +
- Dimitriadis GK, Randeva MS, Miras AD. Potential Hormone Mechanisms of Bariatric Surgery. Curr Obes Rep. 2017;6(3):253-265. doi:10.1007/s13679-017-0276-5
- LOOK AHEAD (2013; NEJM) Weight loss and exercise in T2DM. N Engl J Med. 2013;369:145-154. doi:10.1056/NEJMoa1212914
- Fryar CD, Kruszon-Moran D, Gu Q, Ogden CL. National Health Statistics Reports, Number 122, December 20, 2018.; 1999. https://www.cdc.gov/nchs/data/nhsr/nhsr122-508.pdf. Accessed October 28, 2019.
- Huovinen HT, Hulmi JJ, Isolehto J, et al. Body composition and power performance improved after weight reduction in male athletes without hampering hormonal balance. J Strength Cond Res. 2015;29(1):29-36. doi:10.1519/JSC.0000000000000619
- Dargent J. Isolated food intolerance after adjustable gastric banding: a major cause of long-term band removal. Obes Surg. 2008;18(7):829-832. doi:10.1007/s11695-008-9495-x
- Eid I, Birch DW, Sharma AM, Sherman V, Shahzeer K. Complications associated with adjustable gastric banding for morbid obesity: A surgeon’s guide. Can J Surg. 2011;54(1):61-66. doi:10.1503/cjs.015709
- The ASMBS/NORC Obesity Poll | NORC.org. http://www.norc.org/Research/Projects/Pages/the-asmbsnorc-obesity-poll.aspx. Accessed October 28, 2019.
- Bhaskaran K, Douglas I, Forbes H, Dos-Santos-Silva I, Leon DA, Smeeth L. Body-mass index and risk of 22 specific cancers: A population-based cohort study of 5·24 million UK adults. Lancet. 2014;384(9945):755-765. doi:10.1016/S0140-6736(14)60892-8
- Steenackers N, Gesquiere I, Matthys C. The relevance of dietary protein after bariatric surgery: What do we know? Curr Opin Clin Nutr Metab Care. 2018;21(1):58-63. doi:10.1097/MCO.0000000000000437
- Ahmed K, Penney N, Darzi A, Purkayastha S. Taste Changes after Bariatric Surgery: a Systematic Review. Obes Surg. 2018;28(10):3321-3332. doi:10.1007/s11695-018-3420-8
- Graham L, Murty G, Bowrey DJ. Taste, smell and appetite change after Roux-en-Y gastric bypass surgery. Obes Surg. 2014;24(9):1463-1468. doi:10.1007/s11695-014-1221-2
- Steenackers N, Gesquiere I, Matthys C. The relevance of dietary protein after bariatric surgery: What do we know? Curr Opin Clin Nutr Metab Care. 2018;21(1):58-63. doi:10.1097/MCO.0000000000000437
- Backman O, Stockeld D, Rasmussen F, Näslund E, Marsk R. Alcohol and substance abuse, depression and suicide attempts after Roux-en-Y gastric bypass surgery. Br J Surg. 2016;103(10):1336-1342. doi:10.1002/bjs.10258
- Unforeseen Consequences: Bariatric Surgery Side Effects - Endocrine News. https://endocrinenews.endocrine.org/unforeseen-consequences-bariatric-surgery-side-effects/. Accessed October 28, 2019.
- Neovius M, Bruze G, Jacobson P, et al. Risk of suicide and non-fatal self-harm after bariatric surgery: results from two matched cohort studies. Lancet Diabetes Endocrinol. 2018;6(3):197-207. doi:10.1016/S2213-8587(17)30437-0
- Roberts DC, Pearl N. Meta-analysis of Suicide and Self-harm following Bariatric Surgery. Surg Obes Relat Dis. 2018;14(11):S155-S156. doi:10.1016/j.soard.2018.09.356
- Parlesak A. GASTRIC ALCOHOL DEHYDROGENASE ACTIVITY IN MAN: INFLUENCE OF GENDER, AGE, ALCOHOL CONSUMPTION AND SMOKING IN A CAUCASIAN POPULATION. Alcohol Alcohol. 2002;37(4):388-393. doi:10.1093/alcalc/37.4.388
- Unforeseen Consequences: Bariatric Surgery Side Effects - Endocrine News. https://endocrinenews.endocrine.org/unforeseen-consequences-bariatric-surgery-side-effects/. Accessed October 28, 2019.
- Roberts DC, Pearl N. Meta-analysis of Suicide and Self-harm following Bariatric Surgery. Surg Obes Relat Dis. 2018;14(11):S155-S156. doi:10.1016/j.soard.2018.09.356
- Parlesak A. GASTRIC ALCOHOL DEHYDROGENASE ACTIVITY IN MAN: INFLUENCE OF GENDER, AGE, ALCOHOL CONSUMPTION AND SMOKING IN A CAUCASIAN POPULATION. Alcohol Alcohol. 2002;37(4):388-393. doi:10.1093/alcalc/37.4.388
- Unforeseen Consequences: Bariatric Surgery Side Effects - Endocrine News. https://endocrinenews.endocrine.org/unforeseen-consequences-bariatric-surgery-side-effects/. Accessed October 28, 2019.
- Yuan W, Yu KH, Palmer N, Stanford FC, Kohane I. Evaluation of the association of bariatric surgery with subsequent depression. Int J Obes. 2019. doi:10.1038/s41366-019-0364-6
- Richardson WS, Plaisance AM, Periou L, Buquoi J, Tillery D. Long-term management of patients after weight loss surgery. Ochsner J. 2009;9(3):154-159. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3096273/. Accessed October 28, 2019.
- Biörserud C, Olbers T, Søvik TT, Mala T, Elander A, Olsén MF. Experience of excess skin after gastric bypass or duodenal switch in patients with super obesity. Surg Obes Relat Dis. 10(5):891-896. doi:10.1016/j.soard.2014.01.033
- Wagenblast AL, Laessoe L, Printzlau A. Self-reported problems and wishes for plastic surgery after bariatric surgery. J Plast Surg Hand Surg. 2014;48(2):115-121. doi:10.3109/2000656X.2013.822384
- Cardoso L, Rodrigues D, Gomes L, Carrilho F. Short- and long-term mortality after bariatric surgery: A systematic review and meta-analysis. Diabetes, Obes Metab. 2017;19(9):1223-1232. doi:10.1111/dom.12922
- Bariatric Surgery Misconceptions | ASMBS. https://asmbs.org/patients/bariatric-surgery-misconceptions. Accessed October 28, 2019.
- Courcoulas AP, Belle SH, Neiberg RH, et al. Three-year outcomes of bariatric surgery vs lifestyle intervention for type 2 diabetes mellitus treatment a randomized clinical trial. JAMA Surg. 2015;150(10):931-940. doi:10.1001/jamasurg.2015.1534
- B. W, B. E, M. T, et al. Resting energy expenditure after Roux-en Y gastric bypass surgery. Surg Obes Relat Dis. 2018;14(2):191-199. doi:10.1016/j.soard.2017.10.014 LK - http://findit.library.jhu.edu/resolve?sid=EMBASE&issn=18787533&id=doi:10.1016%2Fj.soard.2017.10.014&atitle=Resting+energy+expenditure+after+Roux-en+Y+gastric+bypass+surgery&stitle=Surg.+Obes.+Relat.+Dis.&title=Surgery+for+Obesity+and+Related+Diseases&volume=14&issue=2&spage=191&epage=199&aulast=Wilms&aufirst=Britta&auinit=B.&aufull=Wilms+B.&coden=&isbn=&pages=191-199&date=2018&auinit1=B&auinitm=
- Tremaroli V, Karlsson F, Werling M, et al. Roux-en-Y Gastric Bypass and Vertical Banded Gastroplasty Induce Long-Term Changes on the Human Gut Microbiome Contributing to Fat Mass Regulation. Cell Metab. 2015;22(2):228-238. doi:10.1016/j.cmet.2015.07.009
- Abu-Gazala S, Horwitz E, Schyr RBH, et al. Sleeve gastrectomy improves glycemia independent of weight loss by restoring hepatic insulin sensitivity. Diabetes. 2018;67(6):1079-1085. doi:10.2337/db17-1028
- Cani PD. Severe obesity and gut microbiota: does bariatric surgery really reset the system? Gut. 2019;68(1):5-6. doi:10.1136/gutjnl-2018-316815
- Who is a Candidate for Bariatric Surgery? | Patients | ASMBS. https://asmbs.org/patients/who-is-a-candidate-for-bariatric-surgery. Accessed October 28, 2019.
- Holst JJ, Madsbad S, Bojsen-Møller KN, et al. Mechanisms in bariatric surgery: Gut hormones, diabetes resolution, and weight loss. Surg Obes Relat Dis. 2018;14(5):708-714. doi:10.1016/j.soard.2018.03.003
- Iannelli A, Gugenheim J. Laparoscopic Roux-en-Y Gastric Bypass, But Not Rebanding, Should Be Proposed as a Rescue Procedure for Patients With Failed Laparoscopic Gastric Banding. Ann Surg. 2005;241(2):383-384. doi:10.1097/01.sla.0000152994.94095.32
- Bariatric Surgery Procedures | ASMBS. https://asmbs.org/patients/bariatric-surgery-procedures. Accessed October 28, 2019.
- Bariatric surgery - Mayo Clinic. https://www.mayoclinic.org/tests-procedures/bariatric-surgery/about/pac-20394258. Accessed October 28, 2019.
- The ASMBS/NORC Obesity Poll | NORC.org. http://www.norc.org/Research/Projects/Pages/the-asmbsnorc-obesity-poll.aspx. Accessed October 28, 2019.
- Maciejewski ML, Arterburn DE, Van Scoyoc L, et al. Bariatric surgery and long-term durability of weight loss. JAMA Surg. 2016;151(11):1046-1055. doi:10.1001/jamasurg.2016.2317
- O’Brien PE, Hindle A, Brennan L, et al. Long-Term Outcomes After Bariatric Surgery: a Systematic Review and Meta-analysis of Weight Loss at 10 or More Years for All Bariatric Procedures and a Single-Centre Review of 20-Year Outcomes After Adjustable Gastric Banding. Obes Surg. 2019;29(1):3-14. doi:10.1007/s11695-018-3525-0
- Sjöström L. Review of the key results from the Swedish Obese Subjects (SOS) trial - a prospective controlled intervention study of bariatric surgery. J Intern Med. 2013;273(3):219-234. doi:10.1111/joim.12012