Key Takeaways
- Elbow pain is usually caused by adding too much weight or doing too many reps or sets too soon, which slowly damages the tendons in your elbow.
- The best way to reduce elbow pain is to modify your workout plan so that you can keep working out without aggravating your elbow (tips on this below).
- If you want to see even faster results, improving your upper body mobility and weightlifting technique and taking some supplements can also help.
Here’s the tale of the injured athlete:
You’re hammering away at your new training plan, and for the first few weeks, you’re getting bigger, stronger, and more confident every day.
Then it happens.
A creeping pain starts to niggle at your elbow.
Like a true, committed athlete, you shrug it off and get back to the coalface, grinding out more reps, sets, and weight.
A few more weeks pass, though, and you’re forced to bend the knee.
Your elbow is injured, your new plan is kaput, and you aren’t sure what to do next.
You turn to the Internet for answers, and get nothing but more questions.
Some say you should just warm up more, try different exercises, or stop being an idiot and go see a doctor.
Others say that you should stick to the old standby of PRICE (pressure, rest, ice, compression, elevation), do some stretches, and take some glucosamine and ibuprofen.
Then, there’s always the S-word—surgery.
Who should you believe?
Well, while the causes of elbow pain are many and hard to pin down, most cases can be fixed with a few simple changes to your training and recovery plan.
In this article, you’re going to learn:
- The most common cause of elbow pain.
- How to prevent getting elbow pain from weightlifting (especially bench pressing).
- How to fix your elbow pain without taking months away from the gym.
To finish it off, you’ll get a 4-step plan for reducing your elbow pain and preventing it from coming back.
Let’s get started.
What Causes Elbow Pain?
To understand what’s causing elbow pain, we need to first look at the structure and function of the elbow joint.
The elbow joint is formed by the intersection of the humerus (upper arm bone), the radius (large forearm bone), and the ulna (small forearm bone).
Here’s what the elbow joint looks like:

And here’s another angle showing the major tendons of the elbow:

The spot where these bones connect is cross-crossed by tendons, ligaments, and muscles, and in between and around these you’ll find fluid-filled sacs called bursae and pads of cartilage.
The elbow joint is also a synovial joint, which means that the cartilage on the ends of the bones is bathed in a lubricating fluid called synovium to reduce friction.
The elbow’s job is to allow the forearm to flex and extend, and it’s involved in all of the most common upper body exercise like the bench press, military press, pull-up, and barbell row.
It’s also involved to a lesser degree in exercises like the deadlift, squat, and lunge, as these exercises put a lot of tension on the arm muscles that cross the elbow joint.
This is also why seemingly innocent exercises, like lunges, can still cause elbow pain.
So, getting back to the question—what causes elbow pain?
Well, we can narrow the answer down to two primary causes:
1. Traumatic injuries.
If you’re grinding out a PR on the bench press, and your elbow pops and sends you into excruciating pain, then chances are good you’ve torn a tendon or ligament and/or dislocated the elbow.
Not pretty, but hey, at least it’s no mystery why it hurts.
Or, maybe you landed hard on your elbow playing sports, and earned yourself a nice case of “popeye elbow,” technically known as olecranon bursitis, which looks like this:

2. Repetitive strain injuries.
Chances are that the reason you’re here is because you don’t know what’s causing your elbow pain.
It doesn’t look any different. It doesn’t feel any different. You didn’t have some catastrophic accident.
It just started hurting one day of its own damn accord.
In this case, chances are good that you’re dealing with a repetitive strain injury (RSI). Repetitive strain injuries are caused by the wear and tear from repeated movement and overuse.
RSIs tend to start small and get progressively worse over time, which leads many people to keep training long after they should have taken time off to heal.
When it comes to elbow pain, some of the most common RSIs include:
1. Lateral epicondylitis. Usually known as tennis elbow, this is caused by the inflammation of tendons that connect to part of the upper arm bone on the outside of the elbow called the lateral epicondyle.
The primary tendon that’s involved is used in movements that involve keeping the wrist straight, which is why it’s often a problem for weightlifters, too.
2. Medial epicondylitis. Usually known as golfer’s elbow, this is caused by inflammation of tendons that connect to part of the upper arm bone on the inside of the elbow called the medial epicondyle.
The primary tendon that’s involved is used in movements that involve flexing the wrist against resistance, which also makes it a common problem for weightlifters.
3. Biceps tendinopathy. This is caused by the inflammation or gradual degeneration of the biceps tendon due to flexing the elbow repeatedly.
4. Radial tunnel syndrome. This is caused by compression of the posterior interosseous nerve, which passes through the elbow joint. It’s less common among weightlifters than other kinds of elbow injury, but still can result from any sport that involves rotating the forearm repeatedly.
5. Elbow bursitis. This is caused by inflammation of the tiny, fluid-filled sacs that pad the elbow joint. There are many small bursae that can become inflamed in the elbow from almost any kind of repetitive movement.
So, which of these is causing your elbow pain?
Well, without the help of a doctor, it’s often hard to pinpoint the exact cause. Even if you get professional help you may never know for sure.
The good news is that even if you don’t know exactly what part of the elbow is hurting, the cause usually boils down to this: overuse injuries.
Overuse and Elbow Pain

In the vast majority of cases, elbow pain is caused by simply doing too much, too soon.
This is why one out of every two high-level tennis players can expect to develop elbow pain at some point in their careers, and why switching from a sedentary lifestyle to suddenly exercising frequently is one of the most common causes of elbow pain.
People who work in jobs that require constantly lifting, moving, and carrying things also have about twice the risk of developing elbow pain as people with more sedentary jobs.
Although weightlifting isn’t the equivalent of hauling pallets for eight hours a day, it can cause pain through similar means.
When it comes to weightlifting, the tendons of the elbow are often the parts that suffer the most from repetitive use.
A tendon is a strip of connective tissue that connects muscles to bones.
Like muscles, tendons can and do grow stronger over time when you progressively overload them with heavier weights over time.
In fact, that’s the only way to make your tendons stronger.
This sword cuts both ways, though.
After a workout, the tendons in your elbow joint are slightly weakened, and they take time to regenerate and grow stronger.
If you put too much load on the tendon too soon, though, then it doesn’t have time to fully recoup its strength, and it starts to hurt.
Elbow Tendonitis vs. Elbow Tendinosis
Now, there are two conditions that can occur when you push your tendons too hard:
- Tendonitis
- Tendinosis
When most people’s elbows hurt, they assume it’s tendonitis.
-itis is a suffix that means inflammation, so tendonitis means “tendon inflammation.”
When the body experiences an injury, it produces an inflammatory response to help repair the damage, which can cause tenderness, swelling, and pain. Usually, this goes away after several days to six weeks of rest.
Tendonitis is often confused with another cause of elbow pain, though, called tendinosis.
-osis is a suffix that means a disorder or pathological state, so tendinosis means “a disordered or pathological tendon.”
More specifically, it refers to the gradual breakdown of the tendon over time.
After each workout, the small amounts of damage fester, eventually reaching a critical point where the body decides “that’s enough, you need to cut it out,” and your elbow starts hurting to make sure you stop messing with it.
This is an important difference, because if your elbow pain is caused by tendinosis rather than tendonitis, solutions aimed at reducing inflammation aren’t necessarily going to solve the underlying problem.
For instance, many of the most common solutions for elbow pain, like non-steroidal anti-inflammatories (NSAIDs), ice, and powerful anti-inflammatory drugs called corticosteroids don’t help the tendon heal (although they can reduce pain for a few days or weeks).
Tendinosis also tends to take much longer to heal than tendonitis. Compared to muscles, skin, and other tissues, tendons have significantly fewer blood vessels, and thus don’t receive as much oxygen and nutrients to heal, grow, and strengthen.
If you catch tendinosis early, then it usually heals after 6 to 10 weeks of rest. Keep pushing through the pain long enough, though, and you could be looking at 9+ months before you can train at full bore again.
The main thing to know is that in most cases of elbow pain, a few days or weeks of rest isn’t enough. If your elbow has been bothering you for several weeks or months, you can expect to have to take a similar amount of time off (if not significantly longer) to heal.
We’ll talk more about how to speed up that process in a moment. First, let’s look at some of the other common solutions for elbow pain.
The Bottom Line
Elbow pain is usually caused by simply doing too much, too soon. Many people assume this leads to tendonitis, and it can, but it often leads to a more severe problem called tendinosis that usually requires several months or more to fully heal.
Bench Press and Elbow Pain
When people experience elbow pain from weightlifting, it’s usually during the bench press.
There are three reasons for this.
First of all, the bench press allows you to move more weight than almost any other upper body exercise. So, all else being equal, this is going to punish your elbows more over time than, say, dumbbell overhead press.
In this case, the solution is simple—make sure you’re only adding 5 to 10 pounds every week, and taking regular deloads when things start to hurt.
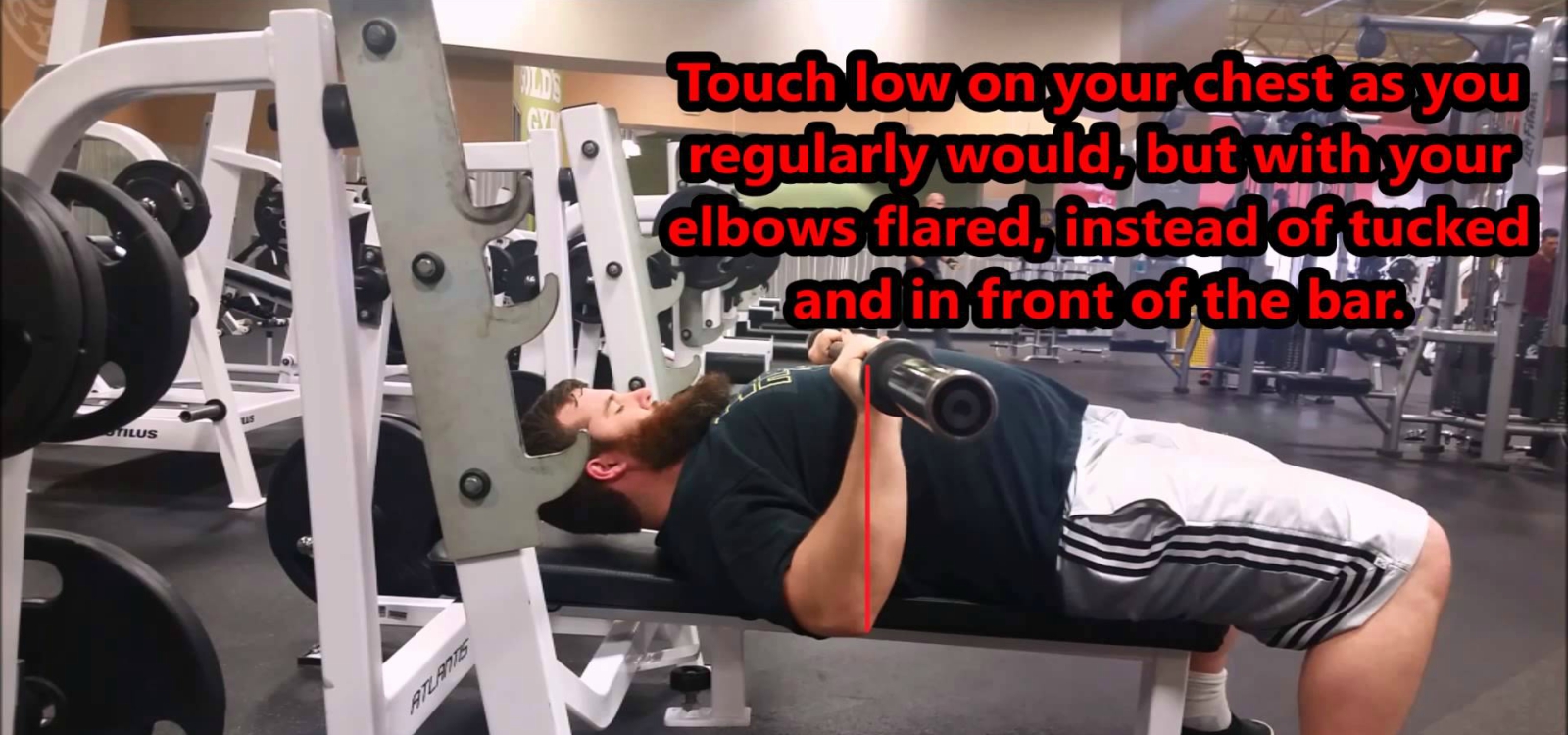
Second, many people have a tendency to keep their elbows close to their sides, also called “tucking” the elbows.
Many fitness gurus even say that this helps prevent shoulder pain, and is thus the proper way to bench.
Here’s what this looks like:

As you can see, this forces the elbow into an awkward position that puts more stress on the tendons around the elbow joint.
Instead, you want your elbows to be more or less directly under the bar, like this:
And if you’re worried about your shoulders, just make sure you aren’t wildly swinging your elbows up past your ears and you’ll be fine.
Thirdly, most people, especially guys, have an almost manic fixation on their bench press. Thus if they’re going to overdo one exercise, the bench is usually it.
It’s also the first exercise many people start with when they’re new to lifting and don’t know proper technique, which means it’s more likely they’ll feel elbow pain on this exercise than, say, overhead press.
All in all, though, there’s nothing about the bench press that makes it uniquely bad for your elbows. Any upper body exercise that involves flexing the elbow can cause pain, especially if you’re throwing around heavy weights, and the solution is usually the same: don’t do too much too soon and deload when needed.
That’s not the only thing you can do, though. Let’s look at exactly what you can do to reduce elbow pain as soon as possible and prevent it from coming back.
The Bottom Line
The main reasons people experience pain when bench pressing are that they’re pressing too much weight too often or too soon, tucking their elbows next to their body, or simply aren’t using proper technique on the whole. Check out this article to learn how to bench properly:
The Easy 4-Step Solution to Reducing Elbow Pain
In most cases, elbow pain from weightlifting is caused by adding too much weight, too many reps, or too many sets too quickly, without enough rest.
That said, the solution isn’t necessarily to stop working out altogether.
Instead, you’re better off modifying and gradually scaling back your workouts so you can keep training while letting your elbow heal.
Here’s how.
Elbow Pain Solution Step 1
Adjust Your Training Plan
In many cases, you’ll only notice elbow pain on certain exercises or variations of exercises.
For example, your elbow might hurt when you barbell bench press, but not when you dumbbell bench press.
If that’s the case, then it’s fine to simply avoid the exercises that hurt until your elbow heals.
This is what people mean when they say they’re “training around an injury.”
Not only does this let you keep training, but research shows that staying active will probably help your elbow heal faster (so long as none of the activities hurt your elbow).
Here’s how to modify your plan while letting your elbow heal:
1. Replace whatever exercise makes your elbow hurt with a similar variation.
For example, if dumbbell rows hurt your elbow, try barbell or cable rows.
If overhead press is the problem, switch to dumbbell overhead press or incline press.
If high-bar squats (which usually require your elbows to be closer together) hurt, then try low-bar squats.
Overuse injuries are usually caused by performing the same movement over and over, so making little adjustments like these is often all you need to give your elbows a break.
If that doesn’t work…
2. Stop doing all heavy compound upper body pressing exercises.
Heavy, compound pressing exercises like the bench press, dumbbell press, and overhead press tend to cause more elbow pain than pulling movements, and taking a break from these often helps.
Instead, do more accessory exercises like dumbbell flyes, cable accessories, or even machines. You can also replace some of your pressing workouts with pulling or leg workouts. (Basically, a push pull legs split without the push workouts.)
If that doesn’t work…
3. Stop doing all upper body exercises.
As much as this sucks, it’s much better than digging yourself into an even deeper hole.
Take at least a month off from upper body exercises or as long as you need to until the elbow pain stops.
4. Stop lifting weights (until your elbow feels better).
If your elbow hurts so much that most upper and lower body exercises are painful, too, then your best bet for recovering as quickly as possible is to stop lifting weights.
Keep moving as much as you can otherwise, but don’t do anything that hurts your elbow.
Some good alternatives are walking, cycling, hiking, golf, rowing, or whatever else you enjoy.
Finally, make sure you aren’t committing any major gym no-nos like skipping your warm up or throwing the weights around with poor form, too.
Elbow Pain Solution Step 2
Improve Your Upper Body Mobility

Improving your upper body mobility probably isn’t going to directly reduce your elbow pain.
It can help, though, if a lack of mobility is keeping you from performing exercises properly.
For example, if your lack of shoulder mobility makes it hard to get your elbows under the bar when benching, then that could be part of the problem.
If you want to learn how to increase your upper body mobility, then check out these articles:
The Definitive Guide to Mobility Exercises: Improve Flexibility, Function, and Strength
How to Improve Shoulder Flexibility and Mobility
Elbow Pain Solution Step 3
Try Physical Therapy
Physical therapy, also called physiotherapy (PT), involves using exercises, special devices, and education to help people regain or preserve healthy movement.
PT can involve any number of different treatments from massage to special movement exercises to medical devices that reinforce proper movement. Different physical therapists also have different methods and recommend different techniques, so it’s hard to say across the board whether it “works” or not.
If resting your elbow doesn’t work, though, then PT is worth a shot.
This is particularly true if you’ve been dealing with elbow pain for a long time and find yourself continually re-injuring your elbow.
As long as the physical therapy sessions are focused on strengthening the injured tendon as much as possible without causing further pain or damage, then it’s likely to help.
Elbow Pain Solution Step 4
Take the Right Supplements
Supplements don’t heal injuries. Training properly, eating a healthy diet, and giving yourself enough (but not too much) rest, does.
Most of the supplements that are commonly marketed for joint pain, like glucosamine chondroitin, have also been largely debunked.
That said, there are safe, natural substances that science indicates may help prevent and reduce elbow pain. (And if you’d like to know exactly what supplements to take to keep you healthy, injury-free, and full of vitality take the Legion Supplement Finder Quiz.)
Let’s quickly review the supplements that are most likely to help.
Fish Oil
Fish oil is known for being anti-inflammatory, and in cases where knee pain is caused by inflammation, taking fish oil may help.
The two main ingredients in fish oil, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), improve the production of anti-inflammatory compounds in the body.
If you eat several servings of fatty fish like salmon, mackerel, sardines, and cod every week, you may not benefit from supplementation with fish oil. If you don’t, however, it’s a good idea to include it in your daily supplement regimen.
And if you’re looking for a high-quality fish oil, then you want to check out Triton.
It’s a high-potency, 100% triglyceride fish oil with added vitamin E to prevent oxidation and rancidity, and natural lemon oil, which prevents noxious “fish oil burps.”
Furthermore, it’s made from sustainably fished deep-water anchovies and sardines and is molecularly distilled to remove synthetic and natural toxins and contaminants.
So, if you want to optimize your mental and physical health and performance and reduce the risk of disease and dysfunction, like shoulder pain, then you want to try Triton today.

Curcumin
Studies show that supplementation with curcumin and black pepper extract reduces inflammatory signals in the joints and, in those with arthritis, relieves pain and stiffness and improves mobility.
When paired with piperine, the clinically effective dosages of curcumin range between 200 and 500 milligrams.
And that’s why there’s 500 mg of curcumin and 25 mg of piperine in each serving of our joint supplement, Fortify.
Fortify contains a clinically effective dose of curcumin in every serving along with three other ingredients also proven to enhance joint health and function:
- Undenatured type ll collagen
- Boswellia serrata
- Grape seed extract
The bottom line is if you want healthy, functional, and pain-free knees that can withstand the demands of your active lifestyle, then you want to try Fortify today.
Undenatured Type ll Collagen
Collagen is the main component of your body’s connective tissues, which means it serves as the primary building block for various things in it, including your skin, teeth, cartilage, bones, and tendons.
The collagen found in supplements comes from the connective tissue in animals, such as cows, chickens, and fish, and while there are over 37 different kinds of collagen in animals, they can be divided into two main categories:
- Type I collagen is the most abundant collagen of the human body, and is present in scar tissue, tendons, ligaments, skin, bones, and more.
- Type II collagen is the collagen that preserves joint function and protects them against damage.
In some cases, your body’s immune system can begin tearing down your own cartilage, in a condition known as arthritis.
Studies show that type II collagen can help alleviate this condition by “teaching” the immune system to stop attacking the proteins in joint cartilage, which in turn can significantly improve joint health and function and decrease or even eliminate pain and swelling.
In other words, type II collagen supplements can work like a natural vaccine of sorts, allowing your body to recognize its own joint collagen as a safe substance, thereby switching off the autoimmune response.
And the best part about type II collagen supplements is that these effects have been demonstrated in people with arthritic conditions and people with healthy joints.
The clinically effective dose of collagen is between 10 to 40 milligrams per day for improving joint health.
That’s a rather large range for dosing, but that’s only because studies have shown benefits using various doses, and it isn’t clear if more is better. Research clearly shows that 10 milligrams is effective, but not that two, three, or four times that amount is necessarily better.
This is why Fortify contains a clinically effective dosage of 10 milligrams of undenatured type ll collagen in every serving.
Grape Seed Extract
Grape seed extract is a substance derived from the ground-up seeds of red wine grapes, which have been used in European medicine for thousands of years.
There are two molecules in grape seed extract that account for most of its health benefits: tannins, which are bitter compounds that make wine taste dry, and procyanidins, which are chains of antioxidants found in some plants.
Much of the research on grape seed extract’s beneficial effects on joint health is extrapolated from research on a similar molecule known as pycnogenol, which is also a potent source of procyanidins. Pycnogenol is significantly more expensive than grape seed extract, however, which is why grape seed extract is preferable for supplementation needs.
The compounds in grape seed extract work by reducing the production of inflammatory compounds in the body, and they also seem to reliably reduce joint pain.
The clinically effective dosage of grape seed extract is 75 to 300 mg per day, which is why Fortify contains 90 mg of grape seed extract per serving.
Boswellia Serrata

Boswellia serrata is a plant that produces an aromatic substance known as frankinsence, which has been used for thousands of years in Ayurvedic medicine to treat various disorders related to inflammation.
Thanks to modern science, we now know why.
Frankinsence contains molecules known as boswellic acids. Research shows that, like curcumin, boswellic acids—and one in particular known as acetyl-keto-beta-boswellic acid, or AKBA—inhibit the production of several proteins that cause inflammation in the body.
And in case you’re wondering, the difference between the anti-inflammatory mechanisms of curcumin and boswellic acids is they work on different enzymes. Curcumin inhibits an enzyme known as cyclooxygenase, or COX, and boswellic acids inbhibit lysyl oxidase, or LOX (and, most notably, 5-LOX).
These anti-inflammatory properties extend to the joints, which is why studies show that Boswellia serrata is an effective treatment for reducing joint inflammation and pain as well as inhibiting the autoimmune response that eats away at joint cartilage and eventually causes arthritis.
The clinically effective dosages of boswellia serrata range between 100 and 200 milligrams.
This is why there is 150 mg of boswellia serrata in each serving of Fortify.
White Willow Bark
White willow bark is similar to aspirin (which is a synthetic version of a chemical that’s also found in willow), that’s been used to reduce pain and inflammation for thousands of years.
It works by blocking the production of inflammatory compounds produced in the body, and it works about as well as other NSAIDs.
The clinically effective dosage of white willow bark is 240 milligrams per day.
Oh, and if you aren’t sure if the supplements discussed in this article are right for your budget, circumstances, and goals, then take the Legion Supplement Finder Quiz! In less than a minute, it’ll tell you exactly what supplements are right for you. Click here to check it out.
The Bottom Line on Elbow Pain
Most of the time, elbow pain is caused by adding too much weight, too many reps, or too many sets too quickly.
It’s that simple.
On the plus side, though, the solution is equally simple—rest.
You don’t want to just stop lifting weights right away, though. Instead, you want to modify your training plan so that you can work around your injury.
There are just four steps:
- Replace whatever exercise makes your elbow hurt with a similar variation.
- Stop doing all heavy compound upper body pressing exercises.
- Stop doing all upper body exercises.
- Stop lifting weights (until your elbow feels better).
If that doesn’t help or if you want to speed up results, then it’s worth improving your upper body mobility, seeing a physical therapist, and, if you feel so inclined, trying a few supplements.
Do that, and chances are good you’ll be back in the gym in a few weeks.
What’s your take on elbow pain? Have anything else to share? Let me know in the comments below!
Scientific References +
- S Chrubasik 1 , O Künzel, A Model, C Conradt, A. B. (n.d.). Treatment of low back pain with a herbal or synthetic anti-rheumatic: a randomized controlled study. Willow bark extract for low back pain - PubMed. Retrieved August 5, 2020, from https://pubmed.ncbi.nlm.nih.gov/11752510/
- Chrubasik, S., Eisenberg, E., Balan, E., Weinberger, T., Luzzati, R., & Conradt, C. (2000). Treatment of low back pain exacerbations with willow bark extract: A randomized double-blind study. American Journal of Medicine, 109(1), 9–14. https://doi.org/10.1016/S0002-9343(00)00442-3
- Kimmatkar, N., Thawani, V., Hingorani, L., & Khiyani, R. (2003). Efficacy and tolerability of Boswellia serrata extract in treatment of osteoarthritis of knee - A randomized double blind placebo controlled trial. Phytomedicine, 10(1), 3–7. https://doi.org/10.1078/094471103321648593
- Sailer, E. R., Subramanian, L. R., Rall, B., Hoernlein, R. F., Ammon, H. P. T., & Safayhi, H. (1996). Acetyl-11-keto-β-boswellic acid (AKBA): Structure requirements for binding and 5-lipoxygenase inhibitory activity. British Journal of Pharmacology, 117(4), 615–618. https://doi.org/10.1111/j.1476-5381.1996.tb15235.x
- Siddiqui, M. Z. (2011). Boswellia serrata, a potential antiinflammatory agent: An overview. In Indian Journal of Pharmaceutical Sciences (Vol. 73, Issue 3, pp. 255–261). Indian J Pharm Sci. https://doi.org/10.4103/0250-474X.93507
- Cisár, P., Jány, R., Waczulíkova, I., Sumegová, K., Muchová, J., Vojtaššák, J., Ďuraćková, Z., Lisý, M., & Rohdewald, P. (2008). Effect of pine bark extract (Pycnogenol®) on symptoms of knee osteoarthritis. Phytotherapy Research, 22(8), 1087–1092. https://doi.org/10.1002/ptr.2461
- Crowley, D. C., Lau, F. C., Sharma, P., Evans, M., Guthrie, N., Bagchi, M., Bagchi, D., Dey, D. K., & Raychaudhuri, S. P. (2009). Safety and efficacy of undenatured type II collagen in the treatment of osteoarthritis of the knee: A clinical trial. International Journal of Medical Sciences, 6(6), 312–321. https://doi.org/10.7150/ijms.6.312
- ML, B., JM, K., EW, S. C., DO, C., D, F., M, W., MJ, F., S, C.-T., E, F., A, M., CH, L., & DE, T. (1998). Treatment of rheumatoid arthritis with oral type II collagen. Results of a multicenter, double-blind, placebo-controlled trial. Arthritis and Rheumatism, 41(2). https://doi.org/10.1002/1529-0131(199802)41:2<290::AID-ART13>3.0.CO;2-R
- Bayrak, Ş., & Mitchison, N. A. (1998). Bystander suppression of murine collagen-induced arthritis by long-term nasal administration of a self type II collagen peptide. Clinical and Experimental Immunology, 113(1), 92–95. https://doi.org/10.1046/j.1365-2249.1998.00638.x
- Clark, K. L., Sebastianelli, W., Flechsenhar, K. R., Aukermann, D. F., Meza, F., Millard, R. L., Deitch, J. R., Sherbondy, P. S., & Albert, A. (2008). 24-Week study on the use of collagen hydrolysate as a dietary supplement in athletes with activity-related joint pain. Current Medical Research and Opinion, 24(5), 1485–1496. https://doi.org/10.1185/030079908X291967
- Lugo, J. P., Saiyed, Z. M., Lau, F. C., Molina, J. P. L., Pakdaman, M. N., Shamie, A. N., & Udani, J. K. (2013). Undenatured type II collagen (UC-II®) for joint support: A randomized, double-blind, placebo-controlled study in healthy volunteers. Journal of the International Society of Sports Nutrition, 10, 48. https://doi.org/10.1186/1550-2783-10-48
- Shoulders, M. D., & Raines, R. T. (2009). Collagen structure and stability. In Annual Review of Biochemistry (Vol. 78, pp. 929–958). NIH Public Access. https://doi.org/10.1146/annurev.biochem.77.032207.120833
- Zdzieblik, D., Oesser, S., Baumstark, M. W., Gollhofer, A., & König, D. (2015). Collagen peptide supplementation in combination with resistance training improves body composition and increases muscle strength in elderly sarcopenic men: A randomised controlled trial. British Journal of Nutrition, 114(8), 1237–1245. https://doi.org/10.1017/S0007114515002810
- Panahi, Y., Rahimnia, A. R., Sharafi, M., Alishiri, G., Saburi, A., & Sahebkar, A. (2014). Curcuminoid treatment for knee osteoarthritis: A randomized double-blind placebo-controlled trial. Phytotherapy Research, 28(11), 1625–1631. https://doi.org/10.1002/ptr.5174
- Jackson, J. K., Higo, T., Hunter, W. L., & Burt, H. M. (2006). The antioxidants curcumin and quercetin inhibit inflammatory processes associated with arthritis. Inflammation Research, 55(4), 168–175. https://doi.org/10.1007/s00011-006-0067-z
- Bost, J., Maroon, A., & Maroon, J. (2010). Natural anti-inflammatory agents for pain relief. Surgical Neurology International, 1(1), 80. https://doi.org/10.4103/2152-7806.73804
- Wilkens, P., Scheel, I. B., Grundnes, O., Hellum, C., & Storheim, K. (2010). Effect of glucosamine on pain-related disability in patients with chronic low back pain and degenerative lumbar osteoarthritis: A randomized controlled trial. JAMA - Journal of the American Medical Association, 304(1), 45–52. https://doi.org/10.1001/jama.2010.893
- Vaquero-Picado, A., Barco, R., & Antuña, S. A. (2016). Lateral epicondylitis of the elbow. EFORT Open Reviews, 1(11), 391–397. https://doi.org/10.1302/2058-5241.1.000049
- Weber, C., Thai, V., Neuheuser, K., Groover, K., & Christ, O. (2015). Efficacy of physical therapy for the treatment of lateral epicondylitis: a meta-analysis. BMC Musculoskeletal Disorders, 16(1), 223. https://doi.org/10.1186/s12891-015-0665-4
- Sorrenti, S. J. (2006). Achilles tendon rupture: Effect of early mobilization in rehabilitation after surgical repair. Foot and Ankle International, 27(6), 407–410. https://doi.org/10.1177/107110070602700603
- Khan, K. M., Cook, J. L., Bonar, F., Harcourt, P., & Åstrom, M. (1999). Histopathology of common tendinopathies: Update and implications for clinical management. Sports Medicine, 27(6), 393–408. https://doi.org/10.2165/00007256-199927060-00004
- Khan, K. M., Cook, J. L., Taunton, J. E., & Bonar, F. (2000). Overuse tendinosis, not tendinitis. Part 1: A new paradigm for a difficult clinical problem. In Physician and Sportsmedicine (Vol. 28, Issue 5, pp. 38–48). McGraw-Hill Companies. https://doi.org/10.3810/psm.2000.05.890
- Tempfer, H., & Traweger, A. (2015). Tendon vasculature in health and disease. Frontiers in Physiology, 6(NOV), 330. https://doi.org/10.3389/fphys.2015.00330
- Mohamadi, A., Chan, J. J., Claessen, F. M. A. P., Ring, D., & Chen, N. C. (2017). Corticosteroid Injections Give Small and Transient Pain Relief in Rotator Cuff Tendinosis: A Meta-analysis. In Clinical Orthopaedics and Related Research (Vol. 475, Issue 1, pp. 232–243). Springer New York LLC. https://doi.org/10.1007/s11999-016-5002-1
- Collins, N. C. (2008). Is ice right? Does cryotherapy improve outcome for acute soft tissue injury? In Emergency Medicine Journal (Vol. 25, Issue 2, pp. 65–68). Emerg Med J. https://doi.org/10.1136/emj.2007.051664
- Enthoven, W. T. M., Roelofs, P. D. D. M., Deyo, R. A., van Tulder, M. W., & Koes, B. W. (2016). Non-steroidal anti-inflammatory drugs for chronic low back pain. In Cochrane Database of Systematic Reviews (Vol. 2016, Issue 2). John Wiley and Sons Ltd. https://doi.org/10.1002/14651858.CD012087
- Bass, E. (2012). Tendinopathy: Why the difference between tendinitis and tendinosis matters. International Journal of Therapeutic Massage and Bodywork: Research, Education, and Practice, 5(1), 14–17. https://doi.org/10.3822/ijtmb.v5i1.153
- Taylor, S. A., & Hannafin, J. A. (2012). Evaluation and Management of Elbow Tendinopathy. Sports Health, 4(5), 384–393. https://doi.org/10.1177/1941738112454651
- Bass, E. (2012). Tendinopathy: Why the difference between tendinitis and tendinosis matters. International Journal of Therapeutic Massage and Bodywork: Research, Education, and Practice, 5(1), 14–17. https://doi.org/10.3822/ijtmb.v5i1.153
- Galloway, M. T., Lalley, A. L., & Shearn, J. T. (2013). The role of mechanical loading in tendon development, maintenance, injury, and repair. In Journal of Bone and Joint Surgery - Series A (Vol. 95, Issue 17, pp. 1620–1628). Journal of Bone and Joint Surgery Inc. https://doi.org/10.2106/JBJS.L.01004
- Viikari-Juntura, E., Kurppa, K., Kuosma, E., Huuskonen, M., Kuorinka, I., Ketola, R., & Konni, U. (1991). Prevalence of epicondylitis and elbow pain in the meat-processing industry. Scandinavian Journal of Work, Environment and Health, 17(1), 38–45. https://doi.org/10.5271/sjweh.1736
- Luk, J. K. H., Tsang, R. C. C., & Leung, H. B. (2014). Lateral epicondylalgia: Midlife crisis of a tendon. Hong Kong Medical Journal, 20(2), 145–151. https://doi.org/10.12809/hkmj134110
- Tosti, R., Jennings, J., & Sewards, J. M. (2013). Lateral epicondylitis of the elbow. In American Journal of Medicine (Vol. 126, Issue 4). Am J Med. https://doi.org/10.1016/j.amjmed.2012.09.018
- Lutz, F. R. (1991). Radial tunnel syndrome: An etiology of chronic lateral elbow pain. In Journal of Orthopaedic and Sports Physical Therapy (Vol. 14, Issue 1, pp. 14–17). J Orthop Sports Phys Ther. https://doi.org/10.2519/jospt.1991.14.1.14